






How your baby is positioned in the belly is a big factor in determining how you give birth. Here is what you can do to ensure your baby is in the right position.
Positions, positions. And there you were thinking that giving birth was just a case of pushing as hard as you can: if only it was that simple!
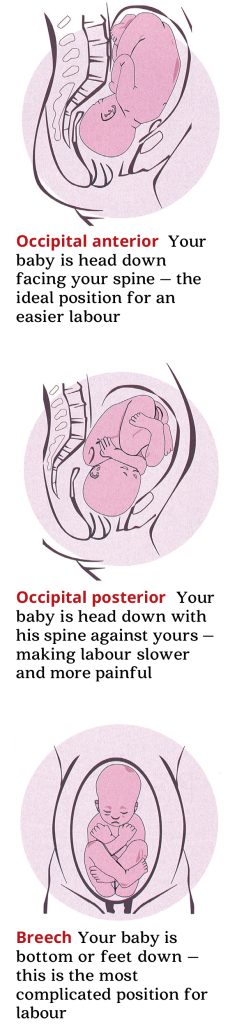
The ideal position for your baby to be in when he is born is called ‘occipital anterior’ – head down with his face towards your spine and his back against your bump. But some babies are in an ‘occipital posterior’ (back-to-back) position – facing your pubic bone and with his spine towards yours.
When a baby is occipital posterior, his chin is lifted slightly from his chest, rather than being flexed (tucked tightly against his chest). A baby’s head is not perfectly round so if his chin is not flexed, the largest part of his head tries to come down the birth canal first, which can slow labour.

Back to Front
Nowadays, more and more babies are posterior at the start of labour – 10 to 15 per cent – and our sedentary lifestyle is partly to blame. Many of us spend the day at our desks and then come home and collapse on the sofa until bedtime.
Spending long periods sitting means that your knees are level with your hips. This tilts your pelvis backwards, so the heaviest part of your baby – his spine – falls towards your back. That is where optimal fetal positioning (OFP) comes in. By sitting upright and leaning slightly forwards, your pelvis tilts forward, giving your baby the space to turn.
Using a gym or birth ball helps you to sit with your hips higher than your knees and rocking gently encourages your baby to move forward. Or try kneeling on cushions and leaning over the ball.
 Keep your posture in mind at all times. At your desk, sit on a cushion with another in the small of your back to keep your hips above your knees. When you are watching TV, sit backwards on a dining chair, with your arms leaning on the backrest. And lie on your left side to help get your baby into the left occipital anterior position, with his head down, facing your spine and to the left side of your bump – it is the best position for birth.
Keep your posture in mind at all times. At your desk, sit on a cushion with another in the small of your back to keep your hips above your knees. When you are watching TV, sit backwards on a dining chair, with your arms leaning on the backrest. And lie on your left side to help get your baby into the left occipital anterior position, with his head down, facing your spine and to the left side of your bump – it is the best position for birth.
An active lifestyle also helps. Swimming on your front also uses gravity to help turn your baby. Be aware, though, that breaststroke can cause back and pelvic pain, so stop if you are uncomfortable. Aquanatal and antenatal yoga are also great.
Try to increase your general activity level, too, and avoid sitting for long periods. Going up and down stairs sideways can help rock your pelvis, nudging your baby into an anterior position, as can alternative therapies, such as shiatsu and acupuncture.
Into the Breech
While delivering a posterior baby can be difficult, a breech (bottom or feet down in the womb) or transverse (lying horizontally) birth is even more complicated. At term, three per cent of babies are breech and less than one per cent are transverse.
The biggest concern here is that your baby may be deprived of oxygen, either because the cord comes out before your baby and is compressed, or because his body delivers but then his head gets stuck. Women with a breech baby at term are usually advised to have a planned C-section.
 With the right advice and support, though, you can deliver a breech baby vaginally.
With the right advice and support, though, you can deliver a breech baby vaginally.
We recommend you deliver in hospital with a team skilled in vaginal breech deliveries. An epidural may be advised, as intervention is often required to help deliver the baby’s head and shoulders.
Before you decide what to do, it is likely you will be offered an external cephalic version (ECV) at 37 weeks, where your bump is manipulated to try to turn your baby. You may be given an injection to relax your uterus, then the obstetrician will apply pressure to your bump to guide your baby into a head-down position.
It is not recommended, however, if your baby is very large or small, or if you are having twins or a planned Caesarean.
An ECV should not be painful, but you may need to keep changing position and have your feet raised so gravity helps your baby turn. Your baby will be monitored; if he becomes distressed, a Caesarean may be needed, but ECV has a 50 per cent success rate.
Burning Issues
Many women prefer to try alternative methods, such as Elkins manoeuvre, where you kneel on your bed with your head, shoulders and upper chest flat on your mattress and your bottom in the air. One study found that spending 15 minutes in this position every two waking hours for five days turned 65 out of 71 breech babies.
The most successful complementary therapy for turning breech babies is moxibustion – where you hold burning moxa sticks, made of dried herb called mugwort, near acupuncture points on your feet.
Having lit the moxa stick, blow it out. Then get your husband to hold the glowing end an inch from your little toe – the acupuncture point – on the outer edge near the cuticle.
It is best to start at 34 weeks and do it twice a day for 15 minutes for both feet. Often the baby turns after six treatments. The success rate is about 66 per cent, though some studies show it to be 92 per cent effective.
Do not try it if you are expecting twins, have a low-lying placenta or high blood pressure, have had any bleeding or have had a c-section in the past. Always consult your doctor first, but if it works, it could help you have a normal delivery.




