By: Associate Professor Dr. Azriyanti Anuar Zaini, Consultant Paediatrician and Paediatric Endocrinologist, University Malaya Medical Centre (UMMC)
Turner Syndrome (TS) affects about ONE in every 2,500 baby girls globally. Find out what parents can do to support their child with TS.
What is Turner Syndrome?
In normal circumstances, genes are carried by chromosomes, which are present in each cell in our body. Every baby girl receives 23 chromosomes from their father and 23 chromosomes from their mother, including one X chromosome from each parent. Therefore, a normal baby girl would have 46 chromosomes with two complete X chromosomes. However, girls with Turner Syndrome have only one X chromosome [45XO].
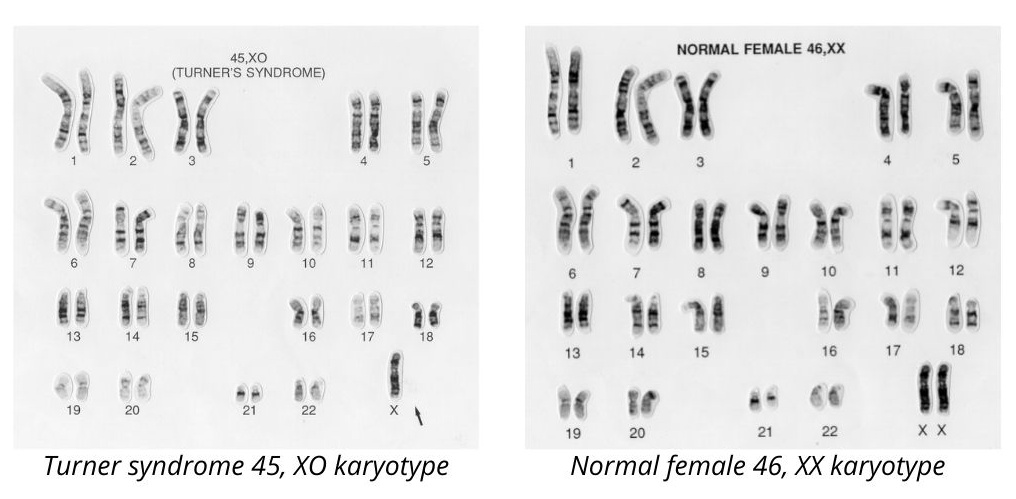
Image via wellcomecollection.org
What are the Signs of Turner Syndrome?
Girls with Turner Syndrome may look like normal children. The most obvious feature that makes them stand out from the rest is that they are really short. In fact, 95 to 100 per cent of girls and young women with Turner Syndrome are much shorter than their peers.1
Girls with Turner Syndrome have other features that may vary from child to child, such as webbed neck, broad chest, pitting nails, low hair line, wide carrying angle or low-set ears.2

webbed neck

Pitting nails
Children with TS may have other associated medical complications, such as congenital heart disease, recurrent otitis media, abnormal kidneys, and scoliosis.2 These physical features can be very subtle, which contributes to why girls with Turner Syndrome are often diagnosed late.
How is Turner Syndrome Treated?
There are treatment options available for children with Turner Syndrome. In Malaysia, the average height of Malaysian women is about 155-157cm. However, for girls with Turner Syndrome, they would only grow up to 130-135cm (20 cm shorter than the average height for Malaysian women).3 This is considered very short for the general population. Being short can predispose them to being disadvantaged and may have an impact to their psychosocial wellbeing.
Turner syndrome girls can be offered growth hormone therapy if deemed suitable by a qualified healthcare professional. Early diagnosis can have a major impact in the treatment outcome. Turner syndrome girls who are treated early may be able to achieve normal adult height.
Other than height, majority of girls with Turner Syndrome may not be able to develop normal pubertal changes. They are at risk of having primary gonadal failure which means that they are unable to have normal menstruation and regular cycle. The doctors (paediatric endocrinologist) will need to investigate this thoroughly and start them on oestrogen replacement therapy gradually to optimise secondary sexual development (e.g., breast and uterine growth). This is done gently over 2-3 years to mimic the normal pubertal changes.
Due to the same reason, women with Turner Syndrome have difficulties to get pregnant in the future. Although currently this is only possible with advanced research facilities, we hope in years to come, reproductive technologies such as In Vitro Fertilisation (IVF) may provide them an option to conceive. On the other hand, pregnancy itself carries a huge risk for women with TS. Maternal complications such as aortic dissection and rupture, hypertension and diabetes can lead to premature deliveries and/or foetal growth restriction.
How is Turner Syndrome Diagnosed?
Turner syndrome can be detected antenatally. High risk pregnancies, advance maternal age and suspicious foetal anomaly are some of the indications for mothers to undergo a special test called the amniocentesis and amniotic blood sampling to test for the foetus karyotype(chromosome). Having said that, upon delivery, babies’ blood is needed to test for karyotyping (chromosome analysis) before Turner syndrome can be confirmed.
Children with turner syndrome may present with2:
- typical neonatal feature (e.g., pitting oedema, dysmorphism, congenital heart disease) **for those presented very early or
- short stature during childhood years or
- primary amenorrhoea during adolescence period
If suspected, a blood test for karyotyping (chromosomal analysis) is needed for confirmation.
What is a Parent’s Role in Detecting Turner Syndrome?
Short stature can be a tell-tale sign of many health problems including Turner Syndrome. Amongst Asians, being short is considered as a norm hence it does not usually spark concern among parents. Lack of awareness and knowledge about TS is mainly why girls with Turner Syndrome are often diagnosed late in Malaysia.
Therefore, we encourage parents to monitor their child’s growth by measuring and tracking their height regularly. Parents may opt to do this with their family doctor or do their own measurements at home. With modern technology, parents can also use the Growth Journey app to track their children’s growth.
What Happens when Your Child is Diagnosed with Turner Syndrome?
Early diagnosis of girls with Turner Syndrome is key to provide timely intervention and improve the prognosis for these children.
When your child is diagnosed with TS, you may need to get more information and plans from your doctor. It is very important for you to follow up with the same doctor who will refer to your child to other subspecialities as necessary. Multidisciplinary care is crucial to ensure your child is receiving the optimal care for their condition.
| Learn more about Turner syndrome by getting a copy of the booklet via this link https://ummctrainings.onpay.my/order/form/book2021. All proceeds from the sale of the Understanding Turner Syndrome booklet will be donated by UMMC to Tabung PPUMCare. |